Working Diagnosis:
Latissimus dorsi tear with complete avulsion of the teres major
Treatment:
The patient underwent open repair of the right latissimus dorsi and teres major. Intraoperative findings found the disruption of both the attachment of the teres major and latissimus dorsi tendon with corresponding avulsion and retraction at the humerus. He was placed in a shoulder immobilizer for the first six weeks following open tendon repair. When the patient was seen by his orthopedic surgeon for six-week postoperative follow up, use of the sling was discontinued, and physical therapy was initiated. The patient-specific physical therapy regimen created by university-affiliated orthopedics and athletic training staff was documented below.
Weeks 0-1:
Gave home exercises post-operatively (including pendulums, elbow ROM, wrist ROM, and grip strengthening)
Remained in shoulder immobilizer for 6 weeks
Weeks 1-6:
Continued home exercises with passive ROM goals 90 degrees forward flexion/30 degrees external rotation at side, abduction max 40-60 degrees without rotation, and grip strengthening
Weeks 6-12:
Began active assistive ROM and active ROM as tolerated
Began light passive stretching at end ranges
Began advanced scapular exercises and progressive resistance exercise for large muscle groups (pecs, lats, etc.)
Began isometrics with arm at side at 8 weeks.
Avoided resisted motions of shoulder until 8-12 weeks post-op
Months 3-12:
Advanced to full ROM as tolerated with passive stretching at end ranges
Advanced strengthening as tolerated with isometrics bands using light weights (1-5 pounds), with 8-12 repetitions per set, with 2-3 sets for rotator cuff, deltoid, and scapula stabilizers, strengthening 3x/week
Began eccentrically resisted motions, plyometrics (weighted ball toss) and proprioception (body blade)
Began sports related rehab at 3-4 months
Returned to throwing at 3-4 months, beginning with light toss
Returned to throwing from the pitcher's mound at 6 months
Returned to full competition at 9-12 months
Outcome:
The patient returned to the affiliated institution for a pre-participation physical. At this visit, the patient had not been given full clearance by his orthopedic surgeon. However, he had returned to the mound for light throwing as he was about 4.5 months from initial surgical repair. The student-athlete reported much improved range of motion and strength with mild restriction and pain at the extremes of external rotation of the right upper extremity.
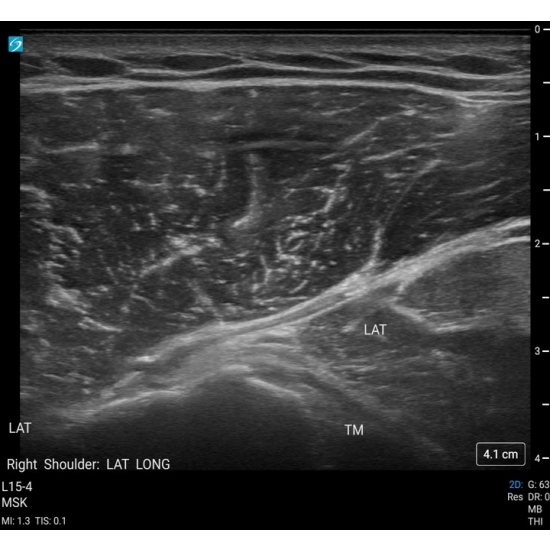
At this time a diagnostic exam of the right shoulder was done also with ultrasound visualization. The biceps tendon, subscapularis and acromioclavicular joint were viewed in both short and long axis. The acromioclavicular ligament was visualized along the long axis. Dynamic motion testing was completed under ultrasound visualization. No signs of subacromial impingement were present. The supraspinatus tendon, infraspinatus tendon, teres minor, teres major, and trapezius were viewed with evidence of mild tendinopathy. The anchor from previous surgical placement was viewed and intact as well.
Case Photo #2
Case Photo #3
The student athlete continued to progress successfully in rehabilitation and returned to throwing protocols with minimal pain and baseline right upper extremity range of motion. He was given full clearance and returned to throwing. The patient continues to be managed by institution affiliated Sports Medicine staff and physician.
Author's Comments:
This case illustrates the intricacies of an infrequent injury including but not limited to injury classification with associated imaging nuances and discussion regarding operative versus conservative management with corresponding return to play/throwing protocols.
Typical shoulder series field magnetic resonance images (MRI) often omit the insertion points of the latissimus dorsi and teres major on the humerus and/or thorax. For complete imaging of associated latissimus dorsi and teres major injuries, the MRI should include muscle belly, myotendinous junction, and insertion of latissimus dorsi and teres minor. More specifically, Chalmers et. al (2021) proposed that the imaging field should "extend to the mid-humerus and the entirety of the scapula" or be ordered as an MRI of the chest wall with "a parasagittal oblique sequence parallel of the posterior chest wall." Fortunately, this student athlete's initial imaging studies viewed the entirety of the latissimus dorsi avulsion and teres major disruption, which is often not the case.
Although there is no generalized consensus regarding the criteria for operative management versus non-operative conservative treatment, this MRI classification seems to be the most unified consensus on injury management. According to Erickson et. al (2017), Grade 1 and 2 latissimus dorsi injuries can be treated with nonoperative, conservative treatment and full thickness tears (grades 3 and 4) are best managed with surgical interventions. Return to sport and throwing outcomes are generally similar between both groups, but, it should be noted that subtypes of injuries (partial tears versus full thickness) were not delineated or reported.
Our athlete's specific return to throwing protocol was university specific and combined an interdisciplinary approach among coaching, medical, and athletic training staff. Given our athlete's success and response, this program can serve as a future model for an in-depth, stepwise, rehabilitation and return to throwing protocol. In conclusion, there is little literature on latissimus dorsi avulsion injuries' incidence and management. Accordingly, return to throwing provides an opportunity for continued discussion to best maximize athlete care and treatment.
Editor's Comments:
This case highlights key diagnostic and therapeutic pearls for a relatively rare injury, latissimus dorsi tear. It adds educational value for those that may not have cared for a patient with this injury or otherwise learned about it, like myself.
In particular, the case provides an excellent example of an MRI that demonstrates the injury, which learners may have never visualized before. Additionally, the author explains how injuries of the latissimus dorsi are sometimes missed when its insertion points are not captured by the MRI. In doing so, the discussion further highlights the value of the diagnostic images provided by the case.
Furthermore, the case provides a detailed and personalized nonoperative treatment regimen on a granular level. The author then discusses medical decision-making, comparing nonoperative and operative treatments, while tying this back to the diagnostic information provided by MRI. In doing so, the author provides readers a framework for the diagnosis and nonoperative treatment of latissimus dorsi injuries.
References:
Friedman MV, Stensby JD, Hillen TJ, Demertzis JL, Keener JD. Traumatic Tear of the Latissimus Dorsi Myotendinous Junction: Case Report of a CrossFit-Related Injury. Sports Health. 2015;7(6):548-552. doi:10.1177/1941738115595975
Pardiwala DN, Subbiah K, Rao N, Modi R. Latissimus Dorsi Tear in an Olympics-Level Tennis Player: Case Report and Review of Literature. Indian J Orthop. 2020;54(3):332-338. Published 2020 Mar 10. doi:10.1007/s43465-020-00055-0
Chalmers, P., Erickson, B., Romeo, A. (2021). Latissimus Dorsi and Teres Major Injuries. Operative Techniques in Sports Medicine. 29. 150805. 10.1016/j.otsm.2021.150805.
Ellman MB, Yanke A, Juhan T, et al. Open repair of an acute latissimus tendon avulsion in a Major League Baseball pitcher. J Shoulder Elbow Surg. 2013;22(7):e19-e23. doi:10.1016/j.jse.2013.03.013
Giberson-Chen CC, Shaw BL, Rudisill SS, et al. Return to Play After Shoulder Surgery in Professional Baseball Players: A Systematic Review and Meta-analysis. Orthop J Sports Med. 2023;11(1):23259671221140853. Published 2023 Jan 11. doi:10.1177/23259671221140853
Erickson BJ, Chalmers PN, Waterman BR, Griffin JW, Romeo AA. Performance and return to sport in elite baseball players and recreational athletes following repair of the latissimus dorsi and teres major. J Shoulder Elbow Surg. 2017;26(11):1948-1954. doi:10.1016/j.jse.2017.05.015
Recker AJ, Gehrman MD, Diaz C, Bullock GS, Trasolini NA, Waterman BR. Baseball Pitchers who Suffer Latissimus Dorsi and Teres Major Tendon Injuries Have a High Return to Play Rate After Either Operative or Nonoperative Treatment. Arthrosc Sports Med Rehabil. 2023;5(5):100787. Published 2023 Sep 9. doi:10.1016/j.asmr.2023.100787
Return To The Case Studies List.



























{kind=link}
{kind=link}